A microRNA gene signature for identification of lung cancer.
 |
Related Articles |
Lung cancer is the leading cause of cancer deaths worldwide, compounded by late diagnosis. MicroRNAs (miRNA) are recently discovered short, noncoding genes that play essential roles in tissue differentiation during normal development and tumorigenesis. miRNA profiles across all histologic grades can provide a reliable and standardized method for the identification of lung cancer.
METHODS: A microRNA lung cancer dataset was analyzed. Differentially expressed microRNAs were obtained post-normalization of data using t-test (p < 0.01). The data for differentially expressed microRNAs were processed using K-nearest neighbors classification method to obtain unique miRNAs expression patterns. The predicted mRNA targets were identified using TargetScan and the molecular functions associated with the predicted targets were retrieved from the Gene Ontology Consortium and represented using GO IDs in a directed acyclic graph.
RESULTS: The results indicate that lung cancer samples can be classified using a small panel of 19 unique microRNAs (8 down-regulated and 11 up-regulated) with over 85% classification accuracy. Furthermore, using classical enrichment analysis, this study identified 66 molecular function groups which are potentially the functional signaling pathways altered by these differentially expressed microRNAs.
CONCLUSIONS: We identified a microRNA gene signature representative of functioning as a diagnostic biomarker for lung cancer. These findings can potentially form the basis for the development of a standardized diagnostic assay that can be used for early diagnosis of lung cancer equally well from resection specimens and cytology samples.

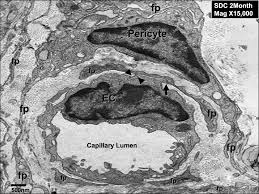 Pericytes are mesenchymal cells embedded within the abluminal surface of the endothelium of microvessels such as capillaries, pre-capillary arterioles, post-capillary and collecting venules, where they maintain microvascular homeostasis and participate in angiogenesis.
Pericytes are mesenchymal cells embedded within the abluminal surface of the endothelium of microvessels such as capillaries, pre-capillary arterioles, post-capillary and collecting venules, where they maintain microvascular homeostasis and participate in angiogenesis. Pneumonia is a life-threatening disease in children. With the current lack of universal diagnostic criteria, the diagnosis is usually made on clinical manifestations and findings from chest radiographs. Ultrasonography has recently been applied to the detection of pulmonary diseases. However, few data have been published showing its effectiveness in detecting pneumonia in children. The objective of this study was to determine the power of lung ultrasonography (LUS) for the diagnosis of pneumonia in children.
Pneumonia is a life-threatening disease in children. With the current lack of universal diagnostic criteria, the diagnosis is usually made on clinical manifestations and findings from chest radiographs. Ultrasonography has recently been applied to the detection of pulmonary diseases. However, few data have been published showing its effectiveness in detecting pneumonia in children. The objective of this study was to determine the power of lung ultrasonography (LUS) for the diagnosis of pneumonia in children.