Ultrastructure of Human Tracheal Smooth Muscle from Asthmatic and Non-asthmatic Subjects: Standardized Methods for Comparison.
 A characteristic feature of asthma is exaggerated airway narrowing, termed airway hyperresponsiveness (AHR) due to contraction of airway smooth muscle (ASM). Although smooth muscle-specific asthma susceptibility genes have been identified, it is not known whether asthmatic ASM is phenotypically different from non-asthmatic ASM in terms of subcellular structure or mechanical function.
A characteristic feature of asthma is exaggerated airway narrowing, termed airway hyperresponsiveness (AHR) due to contraction of airway smooth muscle (ASM). Although smooth muscle-specific asthma susceptibility genes have been identified, it is not known whether asthmatic ASM is phenotypically different from non-asthmatic ASM in terms of subcellular structure or mechanical function.
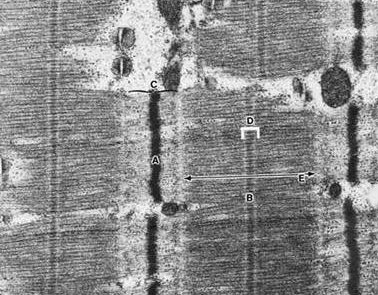
The present study is the first to systematically quantify, using electron microscopy, the ultrastructure of tracheal SM from asthmatic and non-asthmatic subjects. Methodological details concerning tissue sample preparation, ultrastructural quantification, and normalization of isometric force by appropriate morphometric parameters are described. We reasoned that genetic and/or acquired differences in the ultrastructure of asthmatic ASM could be associated with functional changes.
We recently reported that asthmatic ASM is better able to maintain and recover active force generation after length oscillations simulating deep inspirations. The present study was designed to seek structural evidence to account for this observation. Contrary to our hypotheses, no significant qualitative or quantitative differences were found in the subcellular structure of asthmatic versus non-asthmatic tracheal smooth muscle. Specifically there were no differences in average smooth muscle cell cross-sectional area; fraction of the cell area occupied by non-filamentous area; amounts of mitochondria, dense bodies, and dense plaques; myosin and actin filament densities; basal lamina thickness; and the number of microtubules.
These results indicate that functional differences in ASM do not necessarily translate into observable structural changes.
 The efficacy and safety of sublingual immunotherapy in house dust mite-induced asthma have yet to be firmly established. We report the results of a double-blind, placebo-controlled, randomized clinical trial performed in mainland China.
The efficacy and safety of sublingual immunotherapy in house dust mite-induced asthma have yet to be firmly established. We report the results of a double-blind, placebo-controlled, randomized clinical trial performed in mainland China. Asthma remains a major health problem with significant morbidity, mortality and economic costs. In asthma, airway remodelling, which refers to all the microscopic structural changes seen in the airway tissue, has been recognised for many decades and remains one of the defining characteristics of the disease; however, it is still poorly understood.
Asthma remains a major health problem with significant morbidity, mortality and economic costs. In asthma, airway remodelling, which refers to all the microscopic structural changes seen in the airway tissue, has been recognised for many decades and remains one of the defining characteristics of the disease; however, it is still poorly understood.