Novel Aerosol Delivery Devices.
Delivery of medication to sites of action through airways has been used for centuries but has gained momentum in recent decades. Currently available modes of aerosol delivery offer advantages but still there are shortcomings. Delivery of active agents to sites of action is affected by many factors beyond the characteristics of the delivery devices, including the coordination between inhalation and actuation and dependence on the patient's inspiratory flow and breathing pattern.
Recent advances in drug delivery focus around changes in the generation of particle size with better penetration to the targeted sites, easier activation of the device with inspiratory flow, ease of use including fewer steps in using the device, and better portability. Availability of computer chips allows for smart delivery devices to tailor delivery to the patient's breathing pattern and lung function. Further, smart devices can provide feedback to patients.
Novel inhaler technologies, separately or in combination with new therapeutic agents, are in development not only for respiratory diseases but also for diseases of other systems. This article reviews some of the recent clinically relevant advances in aerosol delivery devices.
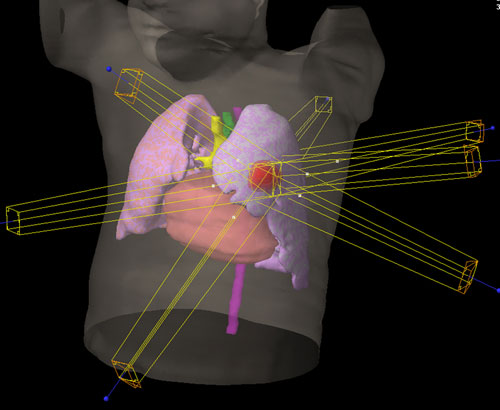 A second lung cancer is occasionally observed in patients who underwent surgical resection of the index lung cancer. The purpose of this study is to evaluate stereotactic body radiation therapy for second lung cancer.
A second lung cancer is occasionally observed in patients who underwent surgical resection of the index lung cancer. The purpose of this study is to evaluate stereotactic body radiation therapy for second lung cancer.
 Video-assisted thoracoscopic surgery is advantageous over traditional surgical practices, because of a faster postoperative recovery period, less pain, and a shorter hospital length of stay. There is no single standard technique in the video-assisted thoracoscopic surgery approach. Although these "minimally invasive" resections are habitually performed through 3-port or 4-port incision, we performed a left lower lobectomy in a 54-year-old male patient for lung cancer, through a 3-cm single-port incision.
Video-assisted thoracoscopic surgery is advantageous over traditional surgical practices, because of a faster postoperative recovery period, less pain, and a shorter hospital length of stay. There is no single standard technique in the video-assisted thoracoscopic surgery approach. Although these "minimally invasive" resections are habitually performed through 3-port or 4-port incision, we performed a left lower lobectomy in a 54-year-old male patient for lung cancer, through a 3-cm single-port incision.