Long-term non-invasive ventilation therapies in children: a scoping review protocol.
| Related Articles |
Non-invasive ventilation (NIV) in children has become an increasingly common modality of breathing support where pressure support is delivered through a mask interface or less commonly through other non-invasive interfaces. At this time, NIV is considered a first-line option for ventilatory support of chronic respiratory insufficiency associated with a range of respiratory and sleep disorders. Previous reviews on the effectiveness, complications and adherence to NIV treatment have lacked systematic methods. The purpose of this scoping review is to provide an overview of the evidence for the use of long-term NIV in children.
METHODS AND ANALYSIS: We will use previously established scoping methodology. Ten electronic databases will be searched to identify studies in children using NIV for longer than 3 months outside an intensive care setting. Grey literature search will include conference proceedings, thesis and dissertations, unpublished trials, reports from regulatory agencies and manufacturers. Two reviewers will independently screen titles and abstracts for inclusion, followed by full-text screening of potentially relevant articles to determine final inclusion. Data synthesis will be performed at three levels: (1) an analysis of the number, publication type, publication year, and country of publication of the studies; (2) a summary of the study designs, outcomes measures used; (3) a thematic analysis of included studies by subgroups.
ETHICS AND DISSEMINATION: This study will provide a wide and rigorous overview of the evidence on the use of long-term NIV in children and provide critical information for healthcare professionals and policymakers to better care for this group of children. We will disseminate our findings through conference proceedings and publications, and evaluate the results for further systematic reviews and meta-analyses.


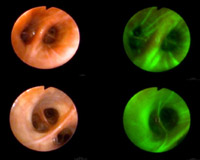 Autofluorescence bronchoscopy (AFB) and computed tomography (CT) enable lung cancer (LC) detection at early (pre-)invasive stage. However, LC risk in individuals harboring pre-invasive endobronchial lesions is unclear. OBJECTIVES To assess LC incidence and identify potential risk determinants in individuals harboring pre-invasive lesions.
Autofluorescence bronchoscopy (AFB) and computed tomography (CT) enable lung cancer (LC) detection at early (pre-)invasive stage. However, LC risk in individuals harboring pre-invasive endobronchial lesions is unclear. OBJECTIVES To assess LC incidence and identify potential risk determinants in individuals harboring pre-invasive lesions.