Smoking-related idiopathic interstitial pneumonia: A review.
 |
For many years, cigarette smoking has been considered as the leading cause of chronic obstructive pulmonary disease and lung cancer. Recently, however, it has also been associated with the development of diffuse interstitial lung diseases. In the latest classification of the major idiopathic interstitial pneumonias (IIP), the term smoking-related IIP has been introduced, including two entities, namely desquamative interstitial pneumonia (DIP) and respiratory bronchiolitis-interstitial lung disease (RB-ILD). Other entities in which smoking has a definite or suggested role include pulmonary Langerhan's cell histiocytosis, smoking-related interstitial fibrosis, combined pulmonary fibrosis and emphysema syndrome and idiopathic pulmonary fibrosis. In this review, we will focus on the mechanisms of smoking-related lung damage and on the clinical aspects of these disorders with the exception of idiopathic pulmonary fibrosis, which will be reviewed elsewhere in this review series.
Prognostic value of variables derived from the six-minute walk test in patients with COPD: Results from the ECLIPSE study.
In addition to the six-min walk distance (6 MWD), other six-min walk test (6 MWT) derived variables, such as mean walk-speed (6MWSpeed), 6-min walk-work (6 MWW), distance-saturation product (DSP), exercise-induced oxygen desaturation (EID), and unintended stops may be useful for the prediction of mortality and hospitalization in patients with chronic obstructive pulmonary disease (COPD). We studied the association between 6 MWT-derived variables and mortality as well as hospitalization in COPD patients and compared it with the BODE index. A three-year prospective study (ECLIPSE) to evaluate the prognostic value of 6 MWT-derived variables in 2010 COPD patients. Cox's proportional-hazard regressions were performed to estimate 3-year mortality and hospitalization. During the follow-up, 193 subjects died and 622 were hospitalized. An adjusted Cox's regression model of hazard ratio [HR] for impaired 6 MWT-derived variables was significant referring to: mortality (6 MWD ≤334 m [2.30], 6MWSpeed ≤0.9 m/sec [2.15], 6 MWW ≤20000 m kg [2.17], DSP ≤290 m% [2.70], EID ≤88% [1.75], unintended stops [1.99]; and hospitalization (6 MWW ≤27000 m kg [1.23], EID ≤88% [1.25], BODE index ≥3 points [1.40]; all p ≤ 0.05). The 6 MWT-derived variables have an additional predictive value of mortality in patients with COPD. The 6 MWW, EID and the BODE index refine the prognosis of hospitalization.
Sputum Bacterial and Fungal Dynamics during Exacerbations of Severe COPD.
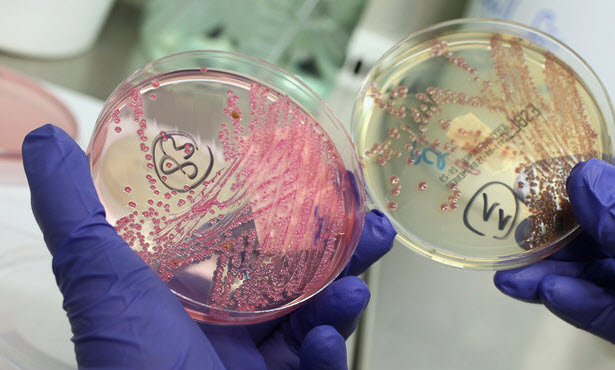 The changes in the microbial community structure during acute exacerbations of severe chronic obstructive pulmonary disease (COPD) in hospitalized patients remain largely uncharacterized. Therefore, further studies focused on the temporal dynamics and structure of sputum microbial communities during acute exacerbation of COPD (AECOPD) would still be necessary.
In our study, the use of molecular microbiological techniques provided insight into both fungal and bacterial diversities in AECOPD patients during hospitalization. In particular, we examined the structure and varieties of lung microbial community in 6 patients with severe AECOPD by amplifying 16S rRNA V4 hyper-variable and internal transcribed spacer (ITS) DNA regions using barcoded primers and the Illumina sequencing platform. Sequence analysis showed 261 bacterial genera representing 20 distinct phyla, with an average number of genera per patient of >157, indicating high diversity. Acinetobacter, Prevotella, Neisseria, Rothia, Lactobacillus, Leptotrichia, Streptococcus, Veillonella, and Actinomyces were the most commonly identified genera, and the average total sequencing number per sputum sample was >10000 18S ITS sequences.
The fungal population was typically dominated by Candia, Phialosimplex, Aspergillus, Penicillium, Cladosporium and Eutypella. Our findings highlight that COPD patients have personalized structures and varieties in sputum microbial community during hospitalization periods.
The changes in the microbial community structure during acute exacerbations of severe chronic obstructive pulmonary disease (COPD) in hospitalized patients remain largely uncharacterized. Therefore, further studies focused on the temporal dynamics and structure of sputum microbial communities during acute exacerbation of COPD (AECOPD) would still be necessary.
In our study, the use of molecular microbiological techniques provided insight into both fungal and bacterial diversities in AECOPD patients during hospitalization. In particular, we examined the structure and varieties of lung microbial community in 6 patients with severe AECOPD by amplifying 16S rRNA V4 hyper-variable and internal transcribed spacer (ITS) DNA regions using barcoded primers and the Illumina sequencing platform. Sequence analysis showed 261 bacterial genera representing 20 distinct phyla, with an average number of genera per patient of >157, indicating high diversity. Acinetobacter, Prevotella, Neisseria, Rothia, Lactobacillus, Leptotrichia, Streptococcus, Veillonella, and Actinomyces were the most commonly identified genera, and the average total sequencing number per sputum sample was >10000 18S ITS sequences.
The fungal population was typically dominated by Candia, Phialosimplex, Aspergillus, Penicillium, Cladosporium and Eutypella. Our findings highlight that COPD patients have personalized structures and varieties in sputum microbial community during hospitalization periods.
Effect of Acute Hypercapnia on Outcomes and Predictive Risk Factors for Complications among Patients Receiving Bronchoscopic Interventions under General Anesthesia.
BACKGROUND: The aim of this study is to investigate the effect of acute hypercapnia on surgery outcomes among patients receiving bronchoscopic interventions under general anesthesia. Furthermore, independent predictive factors for surgery complications were analyzed. METHOD: A total of 323 patients with airway stenosis were enrolled in this retrospective study. Each patient underwent interventional rigid bronchoscopy under general anesthesia. Arterial blood gas (ABG) was measured intraoperatively. In light of PaCO2 levels in ABG, patients were divided into three groups: Group C (control) (PaCO2:≤ 60 mmHg), Group M (moderate) (PaCO2:61-100 mmHg), and Group S (severe) (PaCO2: >100 mmHg). Parameters, including PaO2 levels and recovery delays, were compared across three groups. Complications among patients receiving bronchoscopic interventions were evaluated as well. Independent predictive factors for surgery related complications were analyzed by multivariable regression method. RESULTS: Significant differences in weight (p=0.04), ASA IV (p=0.008), dyspnea index (p=0.003),COPD (p=0.02), dynamic airway collapse (p=0.002), severe stenosis severity (p=0.02), and stenosis locations among three groups were observed. Mild (PaCO2:~60 mmHg) to moderate (PaCO2:60-100 mmHg) hypercapnia was not associated with delayed recovery, whereas severe hypercapnia (PaCO2:>100 mmHg) was associated with delayed recovery, as well as declined PaO2 (p=0.00) and elevated blood glucose levels (p=0.00). The complications of bronchoscopic interventions included postoperative congestive heart failure (14 cases, 4.3%), tracheorrhagia (8 cases, 2.5%), delayed recovery (19 cases, 5.9%), and transfers to ICU after surgery (10 cases, 3.1%). The multivariable regression analysis showed that procedure duration (p=0.003), lobectomy (p=0.007), dynamic airway collapse (p=0.01), severe bronchial stenosis (p=0.01) and hypercapnia (p=0.02) were independent predictive factors for surgery related complications. CONCLUSIONS: Acute hypercapnia lower than 100 mmHg was not associated with detrimental consequences, whereas severe hypercapnia (PaCO2: >100 mmHg) was associated with lower levels of PaO2. Hypercapnia was an independent predictive factor for bronchoscopic intervention complication, which may help physicians to optimize the therapeutic choices.
MACVIA-ARIA Sentinel NetworK for allergic rhinitis (MASK-rhinitis): The new generation guideline implementation.

Several unmet needs have been identified in allergic rhinitis: identification of the time of onset of the pollen season, optimal control of rhinitis and comorbidities, patient stratification, multidisciplinary team for integrated care pathways, innovation in clinical trials and above all patient empowerment. MASK-rhinitis (MACVIA-ARIA Sentinel NetworK for allergic rhinitis) is a simple system centred around the patient which was devised to fill many of these gaps using Information and Communications Technology (ICT) tools and a clinical decision support system (CDSS) based on the most widely used guideline in allergic rhinitis and its asthma co-morbidity (ARIA 2015 revision). It is one of the implementation systems of the Action Plan B3 of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA). Three tools are used for the electronic monitoring of allergic diseases: a cell phone-based daily visual analogue scale (VAS) assessment of disease control, CARAT (Control of Allergic Rhinitis and Asthma Test) and the e-Allergy screening (Premedical system of early diagnosis of allergy and asthma based on online tools). These tools are combined with a clinical decision support system (CDSS) and are available in many languages. An e-CRF and an e-learning tool complete MASK. MASK is flexible and other tools can be added. It appears to be an advanced, global and integrated ICT answer for many unmet needs in allergic diseases which will improve policies and standards. This article is protected by copyright. All rights reserved.