Diagnostic and prognostic value of serum procalcitonin concentrations in primary lung cancers.
 |
Related Articles |
Diagnostic and prognostic value of serum procalcitonin concentrations in primary lung cancers.
Clin Biochem. 2014 Sep 11;
Authors: Patout M, Salaün M, Brunel V, Bota S, Cauliez B, Thiberville L
Abstract
OBJECTIVES: Procalcitonin (PCT) is widely used for the diagnosis of bacterial infections. The aim of this study was to evaluate PCT as a tumor and as a prognostic marker in patients with primary lung cancer.
DESIGN AND METHODS: We retrospectively performed a PCT dosage in the frozen serum samples of 147 patients with pulmonary neoplasia for whom a test of neuron-specific enolase (NSE) had been conducted at the time of diagnosis.
RESULTS: We show that a PCT serum level above 0.15ng/mL was independently linked to the presence of a neuroendocrine component in the tumor (HR=5.809 95% CI [1.695-19.908] p: 0005). Thus, median PCT serum levels were significantly more elevated in small-cell lung cancers than in pulmonary adenocarcinomas: 0.33ng/mL versus 0.07ng/mL (p<0.001). However, the diagnostic value of serum PCT levels for diagnosing carcinoma with a neuroendocrine component remains low (sensitivity 63.8%; specificity 71.9%). In this series, serum PCT levels were significantly more elevated in the presence of liver metastases: 0.37ng/mL versus 0.09ng/mL in the absence of liver metastasis (p<0.001). In uni- and multivariate analyses, a serum PCT level above 0.15ng/mL and the presence of metastases and of sepsis at the time of diagnosis were independent factors of unfavorable prognosis.
CONCLUSIONS: Serum PCT is elevated in patients with lung cancer with neuroendocrine component or with liver metastases. As a consequence, in this population, PCT has a poor specificity for bacterial infection. At diagnosis, an elevated serum PCT is an independent predictive factor of bad prognosis.
PMID: 25218831 [PubMed - as supplied by publisher]

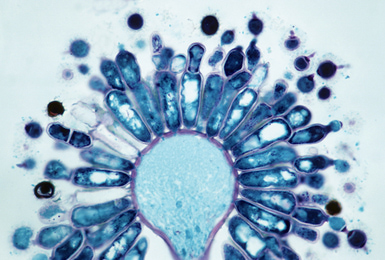 Aspergillus pulmonary infection has traditionally been recognized as a clinical spectrum of increasing pathogenicity, encompassing saprophytic airways colonization historically regarded of doubtful clinical significance, to allergic bronchopulmonary aspergillosis, chronic cavitatory and life-threatening invasive disease in the immunocompromised host. Whilst the latter two categories are rarely encountered in cystic fibrosis (CF), there is recognition of an extending spectrum of disease yet to be reflected in consensus management guidelines. The purpose of this review is to provide an up-to-date overview of this extending spectrum, with a focus on disease categories and their clinical significance.
Aspergillus pulmonary infection has traditionally been recognized as a clinical spectrum of increasing pathogenicity, encompassing saprophytic airways colonization historically regarded of doubtful clinical significance, to allergic bronchopulmonary aspergillosis, chronic cavitatory and life-threatening invasive disease in the immunocompromised host. Whilst the latter two categories are rarely encountered in cystic fibrosis (CF), there is recognition of an extending spectrum of disease yet to be reflected in consensus management guidelines. The purpose of this review is to provide an up-to-date overview of this extending spectrum, with a focus on disease categories and their clinical significance.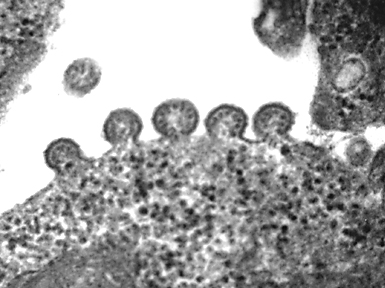 Drug delivery to the airway and lower respiratory tract by aerosol inhalation has become a successful,non-invasive method of preventing and treating local disease of the lung. Consequently, it has been a promising route for clinical trials using highly specific and novel therapies to overcome viral pulmonary infection such as RNA interference, neutralising monoclonal antibodies and microparticle treatments. Yet despite this great potential, this form of delivery has proven somewhat ineffective due to airway remodeling, inflammation and mucus hypersecretion that results from viral symptoms in the respiratory tract.
Drug delivery to the airway and lower respiratory tract by aerosol inhalation has become a successful,non-invasive method of preventing and treating local disease of the lung. Consequently, it has been a promising route for clinical trials using highly specific and novel therapies to overcome viral pulmonary infection such as RNA interference, neutralising monoclonal antibodies and microparticle treatments. Yet despite this great potential, this form of delivery has proven somewhat ineffective due to airway remodeling, inflammation and mucus hypersecretion that results from viral symptoms in the respiratory tract.